Homeless in Vancouver: Fentanyl overdoses are just the beginning
Yesterday (August 31) was the 15th International Overdose Awareness Day. The worldwide harm reduction movement used the occasion to warn that only the widespread adoption of evidence-based strategies—particularly supervised safe-injection facilities—will stem the growing global epidemic of overdose deaths caused by the cheap and ultrapowerful opioid painkiller fentanyl.
What advocates of harm reduction are not warning us about just yet are the eight or nine other synthetic drugs—many of them refinements of fentanyl and almost all of them significantly more potent (or toxic, if you will)—that are just beginning to make their presence felt in street drugs.
For the moment, at least, it’s enough to know that fentanyl-related drug overdoses and overdose deaths are on the rise all over the world, including here in British Columbia. The situation will almost certainly get much worse before it gets better.
And, simply put, when harm-reduction advocates say that supervised safe-injection sites need to be everywhere that the illicit-drug trade is, they know what they’re talking about.
To live and die in B.C.
At North America’s only legal, "low barrier" supervised safe-injection facility—Insite—located in Vancouver’s drug-rich Downtown Eastside neighbourhood, overdoses for the period between January and July of 2016 were 334 percent higher than during the same period 10 years ago, in 2006. This is an astonishing rise, but no one has died from an overdose at Insite in its entire 13-year history—that’s the point of a safe-injection facility.
Outside the walls of Insite, however, users of illicit drugs in British Columbia haven’t fared so well.

(B.C. Coroners Service chart on drug overdoze deaths, 1989 to 2015)
Overdose deaths among British Columbia drug users are, apparently, heading for a new all-time high in 2016, according to figures released in July by the B.C. Coroners Service.
In all of 2015, the coroners service says, there were 505 overdose deaths in the province of British Columbia—the highest number since 1998, if not the highest ever.
But as of July 2016, there have already been 433 apparent illicit-drug overdose deaths in the province. This is a 73.9-percent increase over the same period in 2015 (249) and an average of 61.9 per month. At this rate, with five month to go, 2016 will see more than 742 drug overdose deaths!
The coroner’s service says fentanyl has been a factor in a steadily growing number of overdose deaths, increasing from five percent in 2012 to 30 percent in 2015.
In just the first seven months of 2016, though, fentanyl has been detected in approximately 62 percent of overdose deaths—already more than doubling the percentage from 2015.
In the entire 27-year period covered by the coroner report’s main chart, between 1989 and July of 2016, there have been 6,816 drug-overdose deaths.
Going back four years to 2012, when fentanyl adulteration became an identifiable factor, there have been 1,909 deaths: 28 percent of those deaths in 14.8 percent of the time.
The trouble with fentanyl
Aside from the illegal-drug trade itself and the absence of safe-injection facilities besides Insite, the major culprit behind the increasing overdose-death rate in B.C. is fentanyl; this ridiculously powerful prescription painkiller has, apparently, come to dominate the illicit-drug trade in the province.
Certainly it dominates in Vancouver’s Downtown Eastside, where, according to Insite, Fentanyl was detected in 86 percent of drugs tested during a four-week period between July 7 and August 3.
Cocaine and crystal methamphetamine are now significantly cut with fentanyl and the opioid heroin may simply have been largely replaced by its cheaper and more potent relative.
The problem with fentanyl is twofold: it’s too powerful and it’s too cheap.
The profit and loss of cutting heroin with fentanyl
Back in May, the Vancouver Sun reported that an investigation by its parent company PostMedia found a kilogram of powdered fentanyl could be easily purchased over the Internet from a company in China for US$1,800 (plus $35 for shipping). Payment could be by money transfer or even using Bitcoin. The goods could be shipped in PlayStation or Xbox cartons. or even under diplomatic seal, “which evade(s) all custom checks”.
In Canadian dollars, that kilo of fentanyl cost about $2,386, or $2.38 per gram. Let’s say a gram of heroin on the streets of Vancouver costs $220, as Vice magazine estimates. Even selling the fentanyl gram-for-gram for heroin would give a drug dealer more than a 9,000-percent profit.
But fentanyl is 20 times more potent than heroin, so a very little goes a very long way. A drug dealer could, potentially, make “heroin” out of one part fentanyl and 19 parts of something else, like vitamin B and baby laxative. This could turn a $2,386 investment into upwards of $4 million dollars!
And if the drug dealer is sloppy and some of their buyers get a bit more than one part of fentanyl? Well, some of their buyers will overdose and probably die (even a 10 percent measurement error can be fatal).
But in the messed up world of drug addicts, overdoses can be seen as a sign of drug quality—making addicts want the obviously more potent opioid drug.
Not the last word in dangerously potent opioids
Both as a focus of public-policy discussion around the social harms of illicit drug use and as an actual ingredient in the illegal drugs themselves, fentanyl has become the dominant thing.
Harm-reduction advocates, in particular, have been building up fentanyl as a kind of ultimate strength threat, a sort of doomsday drug (at least that’s the impression I’ve been getting).
However, when I tried to better understand the relative potency of fentanyl to other opioid drugs, I received a real shock.
Far from being the last word in high potency, fentanyl is just the first (and ALMOST the mildest) of a whole slew of superpowerful synthetic opioids that have been developed over the past 56 years, since fentanyl was first synthesized.
Some of these so-called fentanyl analogues are, literally, hundreds of times more potent than original fentanyl. it’s known that at least one of them is behind waves of overdoses in the U. S. Midwest, and it is even suspected that some of these post-fentanyl opioids may be causing some of the overdoses here in Vancouver.
So what are some of these post-fentanyl opioids and what does it mean for overdoses when the illicit drugs are hundreds of times more potent than they are now?
The arms race to be pain-free and comfortably numb
An equianalgesic, or opioid conversion chart, showing relative potency.—Wikipedia
First, a bit of background. Fentanyl is one of a long line of drugs, like opium, morphine, and heroin, that exploit the human body’s built-in endogenous opioid system in order to quickly reduce pain, stress, and anxiety.
Using an opioid drug to fight severe pain is a little like declaring martial law and calling in the army to quell major civil unrest: there’s always the risk that the army won’t leave once order is restored.
By both a brute-force assault on the brain’s pain receptors and large bribes of euphoria-inducing chemicals like dopamine, opioid drugs can quickly and effectively block pain, even as they disastrously overthrow the body’s natural pain-suppression system.
Opioid drugs are so effective at bribing the human body that it can simply stop producing essential natural opioids—which is a major aspect of the physical addiction to opioid drugs.
The opioid effect blocks pain, slows breathing, counters depression, and generally calms us right down.
Although our bodies will not overproduce natural opioid chemicals, there’s nothing to stop us from taking too high a dose of opioid drugs.
In the case of an overdose, the opioid effect in extremis can simply shut off a person’s autonomic breathing reflex altogether and make them too numb and senseless to care.
The good old opiates of the masses
The first opioid (or, to be traditional, opiate) drug was opium, derived as a white sap from the opium poppy, beginning thousands of years ago. Opium yielded morphine (1803), then codeine (1832) and oxycodone (1917). Morphine led to heroin in 1874.
The drugs first derived from extracts of opium in the 1800s, like morphine and heroin. are the original “narcotics”—from the Greek narkotos, meaning to benumb, or make unconscious.
As opposed to opioids like morphine and heroin, which are derived from a plant, fentanyl (first synthesized in 1960) is entirely artificial, like the opioids methadone (1937-1939) and Demerol (1939).
Modern opioids that make fentanyl look like Aspirin
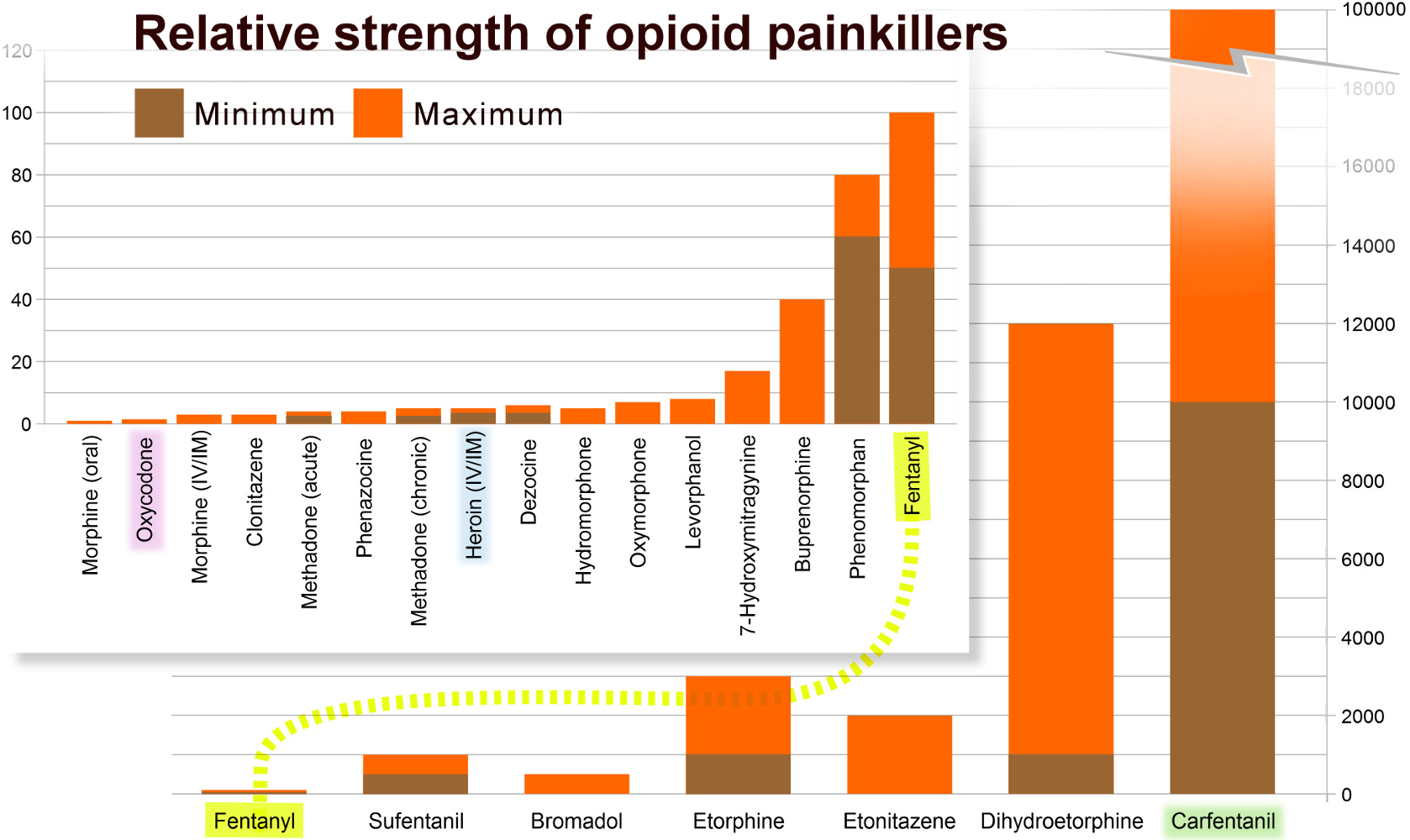
On a scale of opioid potency, if morphine is "one", then heroin is five and fentanyl is 100. But that doesn’t mean that fentanyl is the last word in opioid potency; there are at least eight more opioids that are more powerful still. And a few of them are so absurdly and lethally strong that they make fentanyl look like an over-the-counter headache remedy.
The good news, I suppose, for Vancouver addicts who are dying to use the most potent drugs that their money can buy, is that these more wickedly powerful opioids will inevitably be coming to a street-level drug dealer near them—if they aren’t already here.
Carfentanil, for example, is an opioid elephant tranquilizer developed in 1974 that is at least 100 times more potent than ordinary old fentanyl—falling somewhere between 10,000 and 100,000 on our potency scale. It is already being blamed for a huge spike of overdoses and overdose deaths in the Midwestern U.S. states of Ohio and Indiana. It has also turned up in Kentucky, as well as Florida’s Tampa Bay and Sarasota areas.
In two days in July in Akron, Ohio, 91 people overdosed and eight died from carfentanil.
In Greater Cincinnati, Ohio, where carfentanil is being blamed for a spate of at least 30 overdoses over one August weekend, health officials are warning that carfentanil overdoses are particularly stubborn to treat.
Generally, it takes one injection of the opioid antagonist naloxone to instantly reverse a heroin or a fentanyl overdose, but with carfentanil, “several doses of naloxone may be needed to reverse an overdose,” explained Hamilton County Health Commissioner Tim Ingram.
Western Canada may have dodged sharing the experience of the Midwestern U.S. in early August, when the Canada Border Services Agency (CBSA) intercepted one kilogram of carfentanil that came into Vancouver, B.C., bound for an address in Calgary, Alberta. That kilo potentially represented 50 million fatal doses, the RCMP explained. (This, potentially, works out to something like a billion dollars in street sales.)
There is some question, however, as to whether carfentanil or W-18—a powerful nonopioid painkiller developed in Canada in 1981—may be behind a sudden surge of overdoses last week here in Vancouver.
Insite reported dealing with 26 overdoses between August 23 and 25. This is notably higher than the 15 to 18 ODs that staff expect to see over three typical days. And in a 48-hour period between August 24 and 25, the B.C. Ambulance Service saw 69 calls for suspected overdoses—seven times the average.
Admittedly, August 23, 24, and 25 weren’t typical or average days.
After a five-week wait, Wednesday, August 24, was the day that monthly provincial welfare and disability benefits were finally issued and, anticipating a flood of IV-drug use and the inevitable increase in fentanyl-related overdoses, Insite opened its doors 24 hours a day for the Wednesday, Thursday, and Friday of “welfare week” (charmingly referred to by many in the Downtown Eastside as “Mardi Gras”).
Tellingly however, Darwin Fisher, the manager of Insite, echoed the experience of health-care officials in Greater Cinncinati, when he told CTV News:
“We’ve been having to give three doses of Narcan (the trade name of naloxone), which suggests there is a very potent strain of opiates on the street.”
The elephant (tranquilizers) in the room
Here is a rundown of some of the post-fentanyl opioids—all potential candidates for Mr. Fisher’s “very potent strain of opiates”.
Acetylfentanyl (desmethyl fentanyl) is a synthetic opioid derived from fentanyl but only about 15 percent as potent, which still makes it about three times more powerful a painkiller than heroin. It has no known use, other than as a designer/street drug. In May of 2013, Montreal police seized three kilograms of acetylfentanyl, along with a quantity of the even more potent opioid bromadol. Reportedly, four police officers were intoxicated simply by handling the powerful drugs.
Sufentanil (R30730, branded Sufenta) is another synthetic opioid derived from fentanyl, which is five to 10 times more potent than its parent. Used principally as an anesthetic and for postoperative-pain management, sufentanil is currently the strongest opioid painkiller available for use in humans—in western nations, at least, where all the stronger opioids are approved for veterinary use only.
Bromadol (BDPC) is about five times more potent than fentanyl. It has no therapeutic uses among humans.
Ohmefentanyl is a synthetic fentanyl analogue that has been shown to be 28 times more potent than fentanyl in animal studies. It seems to have no clinical application.
Etorphine (M99) is a semi-synthetic opioid between 10 to 30 times more potent than fentanyl. It is only legally approved for immobilizing large mammals, such as elephants. In animals, its effects are counteracted by diprenorphine; and in humans, by naloxone.
Etonitazene is an opioid variously estimated to be between 10 to 30 times more potent than fentanyl. Wikipedia, however, cites an academic paper saying that its greatest potency only applies to mammals other than people.
Dihydroetorphine is a semisythetic opioid derived from the veterinary painkiller/anesthetic etorphine. It is estimated to be between 10 and 120 times more potent than fentanyl. It is used in China as a painkiller for people.
Lofentanyl is a super-powered fentanyl derivative, about which very little information is available. It’s described in Principles of Forensic Toxicology: Second Edition (2006) as being 6,000 times more powerful than morphine. Despite such inhuman potency, it is used to treat people—specifically, trauma victims. An online PDF document ascribes to it a remarkably long duration of action and a potency slightly greater than carfentanil (which would make it more than 100 times more powerful than fentanyl).
Carfentanil (R 33799, carfentanyl, 4-carbomethoxyfentanyl) is a synthetic opioid that is variously estimated to be between one hundred and one thousand times as potent as its parent opioid, fentanyl. It has been sold under the brand name Wildnil as a general anesthetic for large mammals such as elephants, which is its only legal use.
It’s as accurate to say that drugs take the addicts
For many of the people addicted to hard drugs, taking them at least started out as a choice; for a surprising number of others, it was a prescription opioiod analgesic, for a serious injury or chronic pain, that led them to unexpected addiction.
It shouldn’t matter, though, how people come to drug addiction.
It’s just wrong to penalize, criminalize, or ostracize anyone for not being inhumanly strong enough to beat a physical drug addiction. Blame laid on addicts is misplaced. The real crimes are committed by the illicit-drug trade, which knowingly and deceptively sells dangerous substances that are intended to financially enslave the unwitting for as long as it doesn’t kill them.
Addicts are the duped victims. And governments are also victimized—by the cost in harms and lives that the illicit-drug trade imposes on society.
In a way, though, the phenomenon of drug addiction represents a real failure on the part of governments to fulfill their classical purpose, which is to protect citizens.
Governments must not repeat past negligence
The nonreaction of many governments around the world to the toxic opioid contamination of the illicit-drug supply, arguably, has some parallels to the 1980s, when many companies and governments initially turned a blind eye to screening blood products for contamination. This led to tens of thousands of hemophiliacs being infected with HIV and hepatitis C.
It also led to many deaths and lawsuits.
In Canada, where about 2,000 people were infected with HIV and up to 60,000 with hepatitis C, the Canadian Red Cross was ultimately found guilty by the Supreme Court of Canada of negligence for failing to effectively screen blood donors.
Governments that turn a blind eye now to the clear trend of overdose deaths are not just being negligent. If they do not begin to adopt proven harm-reduction policies toward illicit-drug use, in my opinion, they risk actual complicity with the deaths to come.
Governments that do not act will, in effect, be standing aside and allowing the illicit-drug trade to get away with murder—mass murder, actually—of many thousands of people who simply made an unlucky choice.
Make supervised safe injection the rule rather than the exception—not to mention evidence-based drug treatment.
End the life-and-death fentanyl lottery before it gets worse.













Comments