Battling a fentanyl crisis, B.C. quietly expands access to clean drugs that addicts can substitute for heroin
The province plans to make prescription heroin more widely available, not only to treat severe addictions, but also to save people from the fentanyl crisis and overdose deaths
The Portland Hotel Society (PHS) has quietly forged ahead with a lifesaving but controversial tool that could help alleviate Vancouver’s fentanyl crisis.
In December 2016, Dr. Christy Sutherland began prescribing hydromorphone to one patient who for many years struggled with a severe addiction to heroin.
Hydromorphone, which sells under the brand name Dilaudid, is a synthetic opioid very similar to heroin that is routinely used in hospitals across Canada to treat severe pain. Sutherland, a staff physician for PHS, prescribed the drug off-label for the purpose of managing the man’s addiction to opioids.
Every day, two times a day, Sutherland sees that patient at Pier Pharmacy on Main Street and gives him hydromorphone via an injection. As a result, he stopped buying illegal heroin from street dealers. That means he no longer risks his life by injecting unknown substances that likely contain fentanyl, the synthetic opioid that was associated with hundreds of deaths in B.C. last year.
The patient also no longer has to steal to raise enough money to feed his habit, because the program—called injectable-opioid-agonist treatment—is covered by PharmaCare. He has largely left behind the chaos that comes with feeding an addiction illegally.
Since enrolling that first patient (PHS declined to name him for privacy reasons), Sutherland has expanded the Downtown Eastside nonprofit’s hydromorphone program to 19 other people who were diagnosed with an addictions disorder.
PHS executive director Jennifer Breakspear said the organization is not doing interviews about the program at this time, but she wrote in an email: “That number will grow when we’re ready to launch the full program.”
Following Europe's example
Injectable-opioid-agonist treatment has been available in Europe for decades. It is prescribed to treat long-time addictions where people have repeatedly failed with more traditional treatments such as methadone. But Sutherland is one of very few doctors in North America to prescribe hydromorphone for the treatment of an addiction. The first was Dr. Scott MacDonald, who works at Crosstown Clinic, which is located just down the street from PHS, at the intersection of East Hastings and Abbott streets. In November 2014, Crosstown became the first health-care facility in North America to administer hydromorphone and prescription heroin outside of a clinical trial. Today there are about 90 long-time opioid addicts who receive prescription heroin there, plus another 20 who receive hydromorphone.

According to documents the Straight obtained through freedom-of-information requests, the B.C. government has been working to expand access to programs like Crosstown Clinic’s since late 2016. Morover, it plans on doing so not only to treat severe addictions—for which opioid-agonist treatment is used in other parts of the world—but also to save people from the fentanyl crisis and overdose deaths.
A November 29 email shows that Dr. Patty Daly, chief medical health officer for Vancouver Coastal Health, inquired about costs at Crosstown because, according to a VCH staffer, she “wants to know as the MOH [Ministry of Health] is thinking of using a Crosstown model to address the OD crisis”.
In addition, on December 7, Dr. Brian Emerson, a consultant working for the Ministry of Health, emailed high-level officials working for B.C.’s regional health-care providers to inform them that the government was discussing an expansion of opioid-agonist treatment in response to B.C.’s sharp rise in illicit-drug overdose deaths.
“As you know expansion of injectable opioid agonist treatment (diacetylmorphine and hydromorphone – iOAT), potentially augmented with slow-release oral morphine (SROM) is being considered as part of the response to the overdose emergency,” Emerson wrote.
He asked for suggestions for where the health authorities might establish opioid-agonist treatment programs or integrate them into existing health-care locations, and for recommendations on any specific physicians who might be willing to provide the treatment.
Also on December 7, a “stakeholders meeting” was held at St. Paul’s Hospital on the subject of “supervised injectable treatment”. An agenda obtained by the Straight states that the purpose of the meeting was to “Move the conversation forward among stakeholders” and to “find ways to accelerate actions in light of the current overdose crisis”.
Last year in B.C., 935 people died of an illicit-drug overdose, up from 518 the previous year. Fentanyl was detected in 45 percent of those deaths. From 2001 to 2010, the average number of fatal overdoses in B.C. each year was 204.
Expanding access beyond Vancouver
In a telephone interview, B.C.’s provincial health officer, Dr. Perry Kendall, confirmed that B.C. is working to expand access to prescription heroin. But he cautioned that likely won’t happen for some time. Therefore, Kendall said, the immediate priority is hydromorphone.
He explained that this is because it is very difficult for a doctor to offer heroin, which is prescribed under the medical name diacetylmorphine.
There is no domestic producer of diacetylmorphine in Canada, so every dose has to be imported from Europe. Getting the drug through customs remains a complicated task. Prescribing diacetylmorphine also requires a Special Access Program request and Health Canada approval for every single patient. In addition, there are stringent security requirements that a clinic must meet to store and distribute diacetylmorphine.
Hydromorphone, on the other hand, is widely available across Canada and can be prescribed without any additional permission from a higher level of government.
“Health Canada is working on making it less of a logistical nightmare for diacetylmorphine,” Kendall said. “I am optimistic that at some point in the not too distant future, we will also be adding diacetylmorphine to the injectable-opioid-substitution program.”
In the meantime, Kendall said, B.C. is moving ahead with hydromorphone.
In addition to PHS providing access to hydromorphone in the Downtown Eastside, Providence Health Care—a nonprofit that operates health-care facilities in partnership with VCH—confirmed it is discussing integrating a prescription-heroin and hydromorphone program into infrastructure at its St. Paul’s Hospital in Vancouver’s West End.
Dr. Victoria Lee is chief medical health officer for Fraser Health Authority, the regional provider responsible for most of the Fraser Valley. She told the Straight that outside of the City of Vancouver, the second municipality to offer this treatment is very likely going to be Surrey.
“We are looking at what population is affected and are in early stages of discussion and planning in terms of what kind of model might work within out setting and where potential expansion opportunities might be,” Lee said. “Really early stages, but we have pulled together some folks to start to look at those details.”
Lee echoed Kendall’s concerns for diacetylmorphine, agreeing that import restrictions for heroin and Health Canada’s complicated requirements for prescribing the drug make hydromorphone the better option for now.
“We are currently working on expanding access to diacetylmorphine but focusing on hydromorphone as an immediate area that we can look at,” Lee said.
Evidence-based treatment
Kendall emphasized that even though expanding access to hydromorphone will be significantly simpler than it would be for prescription heroin, there are still challenges.
The effects of hydromorphone wear off relatively quickly, at which point a patient begins to suffer symptoms of withdrawal. Most patients require three doses of the drug every single day. Delivering opioid-agonist treatment is, therefore, a resource-intensive undertaking.
“We need a pharmacy that holds the drug, and then we need a clinic to do it in,” he explained. “Will it be a supervised-consumption site or will it be an existing clinic that is already offering addictions services?”
The B.C. Centre on Substance Use is currently revising guidelines for the treatment of opioid addictions to include injectable options such as Crosstown Clinic’s prescription-heroin program and PHS’s hydromorphone program.
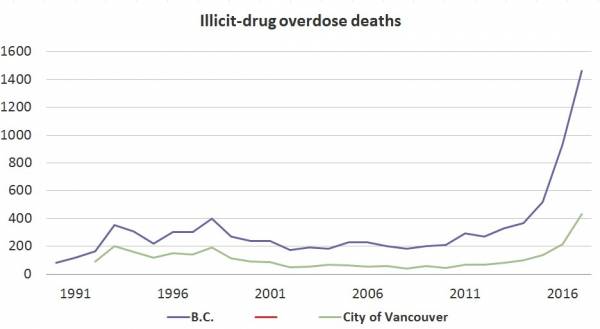 Travis Lupick / B.C. Coroners Service
Travis Lupick / B.C. Coroners Service The off-label use of hydromorphone to treat an opioid addiction gained attention in B.C. in April 2016 when Vancouver researchers published a paper that said the drug can significantly reduce a long-time addict’s propensity to purchase heroin on the street.
For the study, 102 randomized patients were put on diacetylmorphine and 100 were given hydromorphone. Before entering the trial, participants in both groups were addicted to opioids for an average of longer than 15 years. The average number of days they used street heroin during the previous month was about 25. After six months enrolled in the study, the group given diacetylmorphine reported using street heroin an average of 2.64 days during the previous month, and the group put on hydromorphone said they had used street heroin 4.08 days during the previous month.
The paper, published in the Journal of the American Medical Association Psychiatry, concludes: “In jurisdictions where diacetylmorphine is currently not available or for patients in whom it is contraindicated or unsuccessful, hydromorphone could be offered as an alternative.”
Kendall noted the treatment is cost-effective. He explained that while the price of opioid-agonist treatment for one patient is about $24,000 a year, if left outside of the health-care system, that same individual will cost taxpayers between $40,000 and $50,000 a year in police and hospital expenses.
“It’s cost-saving, overall,” he said.
More












Comments